AGACNP Preceptor Matching for Purdue Global Students
The Adult-Gerontology Acute Care Nurse Practitioner track is the hardest of the four Purdue Global NP tracks to place, and it is not close. Acute-care preceptors work in hospitals, ICUs, step-down units, and hospitalist services where access is tightly controlled, schedules are unforgiving, and credentialing is strict. We are an independent clinical-placement service. We are not Purdue University, Purdue Global, or the CCNE. What we do is source an acute-care preceptor who fits your AGACNP requirements and drive the affiliation paperwork through to a signed agreement, working alongside you and your Clinical Student Manager.
What the Purdue Global AGACNP track asks of you
The AGACNP track is an MSN delivered with 100 percent online coursework and a local, in-person practicum you complete in your own region. The classroom part is flexible. The clinical part is not, because acute-care competencies can only be built at the bedside in a setting that treats acutely and critically ill adult and older-adult patients.
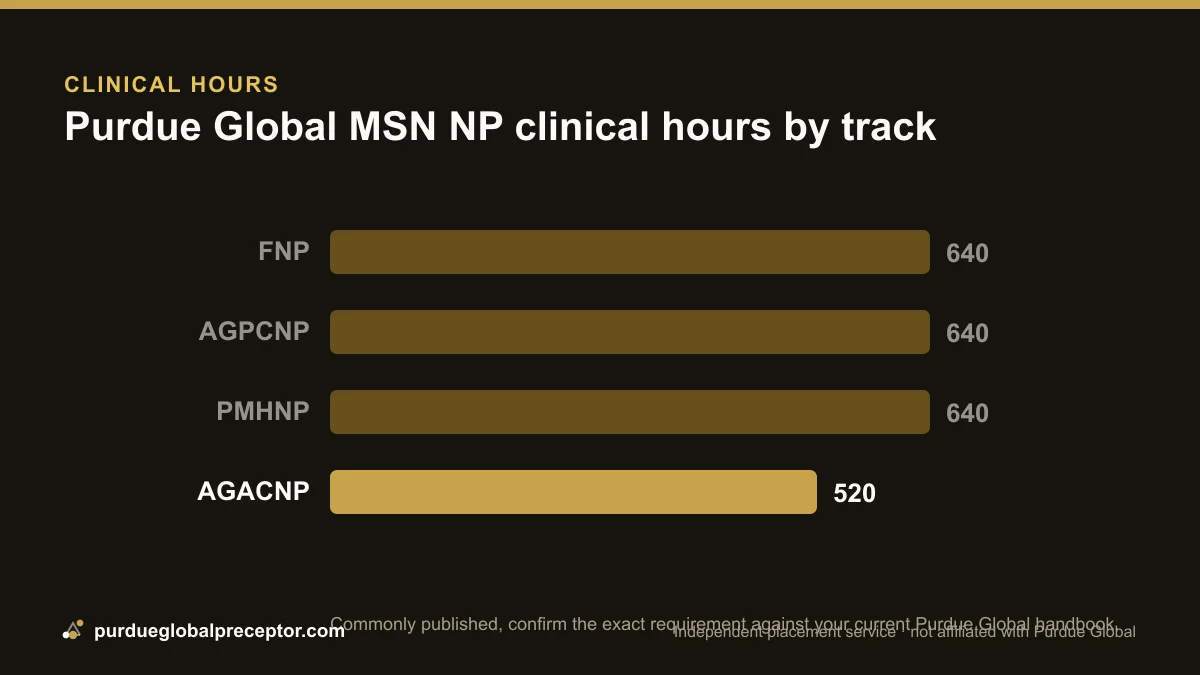
The clinical-hour figure commonly published for this program is 520 hours, which is lower than the 640 hours associated with the FNP, AGPCNP, and PMHNP tracks. We hedge that number deliberately: 520 is the figure we see published for AGACNP, and it is the kind of detail that can change between handbook revisions or differ for post-master's certificate students. Treat it as a planning anchor only. We confirm the exact requirement against your current Purdue Global handbook before you commit to a site, because in acute care a hundred-hour difference can mean the gap between one rotation and two.
Under Purdue Global's model the student carries the lead advocate role for finding clinical sites and preceptors, backed by the University and an assigned Clinical Student Manager. For a clinic-based track that division of labor is manageable. For AGACNP it strains, because the clinicians qualified to precept you sit inside hospital systems whose education offices simply do not respond to a single student's email. The point of bringing in an independent service here is to absorb that hospital-facing burden: you keep the advocate role on paper, and we carry the outreach, the acuity screening, and the agreement push that would otherwise leave you negotiating with a health system on your own.
Purdue Global runs on a quarter-credit system and is accredited by the Higher Learning Commission at the institutional level, with the nursing program accredited by the CCNE. None of that changes the clinical requirement, but it shapes how your terms are structured, so we plan your placement around your actual quarter calendar rather than a generic semester.
Where AGACNP clinical hours are completed
Acute care is defined by the acuity of the patient, not the name on the building. Your AGACNP hours need to be earned in settings where you manage adults and older adults with unstable, complex, or critical conditions. That typically means one or more of the following:
- Intensive care and critical care units, medical, surgical, cardiac, or mixed ICUs where you build invasive-line, ventilator, and rapid-decompensation management exposure
- Hospitalist and inpatient medicine services, admitting, rounding, and managing the acute inpatient population alongside an NP or physician hospitalist
- Step-down and progressive care units, the bridge between ICU and the floor, with telemetry and higher-acuity monitoring
- Emergency departments, undifferentiated acute presentations, stabilization, and disposition decisions
- Specialty acute services, cardiology, pulmonology/critical care, nephrology, trauma, or surgical services that carry an acute inpatient load
A primary-care clinic, a retail health setting, or a low-acuity outpatient office will not satisfy AGACNP competencies even if a willing preceptor works there. We screen every potential acute placement against the track before we propose it, so you don't burn a term in a setting that won't count. If your interest sits closer to clinic-based adult-gero medicine, the AGPCNP primary care track is a different path with different sites.
Why acute preceptors are the scarcest to place
There are simply fewer AGACNP-qualified preceptors than primary-care ones, and the ones who exist are inside systems that limit student access on purpose. Hospital NPs and intensivists carry high patient loads, their hours are shift-based and unpredictable, and many work under contracts that restrict precepting unless the system formally approves it. A preceptor can be willing and still be blocked by their employer.
Acute settings also gate students harder. Hospital credentialing offices, infection-control rules, and risk-management policies add steps that an outpatient clinic never requires, and many large systems route every student through a single education office that prioritizes their own affiliated programs first. Demand makes it worse: acute-care NP students from many programs compete for the same narrow pool, and the slots fill early.
The practical takeaway is timing. Because AGACNP placements are competitive and the upstream paperwork is slower, the single biggest predictor of a smooth rotation is how early you start. Students who reach us a full term ahead have room to work through both the sourcing and the signatures; students who reach us weeks before a rotation are competing for whatever is left. If you want the mechanics of the broader process, see how it works.
How we source an acute preceptor for you
We start from your region, your track, and your quarter calendar, then work outward through acute-care channels rather than generic clinic lists. We approach hospital-employed NPs, intensivists, hospitalist groups, and specialty services directly, and we frame the request the way a busy acute clinician actually evaluates it: scope, supervision load, and whether the affiliation paperwork is already handled.
Because acute preceptors are scarce, we don't hand you a single name and hope. We work multiple leads in parallel, confirm that each setting matches AGACNP acuity, and verify the preceptor's licensure and willingness before we put a placement in front of you. You stay the lead advocate on record with Purdue Global, but you are not the one cold-calling an ICU.
Throughout, your Clinical Student Manager stays in the loop alongside us, not bypassed. Think of it as a clear split of lanes: the CSM holds the formal Purdue Global side, approvals, documentation standards, and what the University will accept, while we run the acute-care sourcing and the desk-to-desk legwork outside it. Acute placements come apart when those two lanes drift; keeping them synchronized, with you copied on what matters, is most of what gets a hospital rotation across the line on time.
Why acute-care agreements take longer
Finding a willing acute preceptor is only half the job. Before you can log a single hour, the clinical site and Purdue Global need a signed clinical affiliation agreement, and in hospital systems this is where placements most often stall.
The slowdown is structural, not personal. A hospital affiliation agreement routes through legal counsel, the system's office of risk management, and frequently a credentialing or graduate-education committee that meets only on a set cadence, see the full agreement timeline and what it covers for the detail. That is the core reason acute sites run on the slower end of the range while an established outpatient practice can turn the same paperwork around quickly; the document itself is similar, but the number of desks it has to cross is not.
Two things follow from that. First, an existing agreement is worth more in acute care than anywhere else, because it lets you skip the committee queue entirely, so the first question we ask of any hospital target is whether it already holds a Purdue Global agreement. Second, when a new agreement is unavoidable, the only lever that matters is lead time: opening the conversation between the system and the University the moment a placement looks viable, rather than waiting for a verbal yes from the preceptor, can be the difference between starting on schedule and pushing a term.
We manage that process with you end to end: checking each target for an existing agreement, routing a new request to the right office instead of a general inbox, and following the document through every signature until it is executed. Acute settings also front-load compliance more than clinics do, background check and immunization clearance plus hospital-specific onboarding such as badging, EHR access, and unit orientation must all be finished before your first shift, so we start those clocks in parallel with the agreement rather than after it.
Other Purdue Global NP tracks we place
AGACNP is the toughest placement, but it is one of four Purdue Global NP tracks we support. If you are weighing your options or precepting in a different specialty, these are the related paths:
- FNP preceptor, Family Nurse Practitioner, the broadest primary-care track
- AGPCNP preceptor, Adult-Gerontology Primary Care, clinic-based adult and older-adult medicine
- PMHNP preceptor, Psychiatric Mental Health, a separate scarce specialty with its own sourcing challenges
Post-master's certificates exist in all four tracks, and the clinical and agreement mechanics are the same. Whichever track you are in, the work is identical in shape: source the right preceptor, confirm the setting fits, and get the affiliation agreement signed in time. For acute care, we simply start that work sooner. When you are ready, tell us your track and region and we'll begin.
Good to know
How many clinical hours does the Purdue Global AGACNP track require?
520 hours is the figure commonly published for this program, notably fewer than the 640 hours tied to the FNP, AGPCNP, and PMHNP tracks. We hedge this because it is the figure we see published and is the kind of detail that can vary between handbook revisions or for certificate students. We confirm the exact requirement against your current Purdue Global handbook before you commit to a site.
Why are AGACNP preceptors harder to find than other NP preceptors?
There are fewer acute-care-qualified preceptors, and most work inside hospital systems that tightly control student access. Hospital NPs and intensivists carry heavy loads, work unpredictable shifts, and often need formal employer approval to precept. Add credentialing, infection-control, and risk-management steps that outpatient clinics don't require, plus competition from many programs for the same slots, and AGACNP becomes the most competitive of the four tracks to place.
What settings count for AGACNP clinical hours?
Hours must be earned where you manage acutely and critically ill adults and older adults: ICUs and critical care units, hospitalist and inpatient medicine services, step-down or progressive care units, emergency departments, and acute specialty services like cardiology, pulmonology/critical care, or trauma. Low-acuity outpatient or primary-care settings will not satisfy AGACNP competencies. We screen every placement against the track before proposing it.
How long does the hospital affiliation agreement take?
When a site already holds an agreement with Purdue Global, it is usually about two to four weeks. A brand-new site that must negotiate one from scratch typically takes about one to two months, and sometimes longer, because hospital legal and risk teams review every clause. We identify which situation applies, open the conversation early, and track the document until it's signed.
Do you work with my Purdue Global Clinical Student Manager?
Yes. Purdue Global asks you to be the lead advocate for your own placement, supported by the University and a Clinical Student Manager (CSM). We do that advocacy with you: the CSM owns the University relationship while we source the acute-care preceptor and move the affiliation paperwork. You remain the student of record. We are an independent service and are not affiliated with or endorsed by Purdue Global, Purdue University, or the CCNE.
When should I start arranging an AGACNP placement?
As early as you can, earlier than for any other track. Acute preceptors are scarce, slots fill ahead of time, and large systems are both the most willing to precept and the slowest to sign agreements. Coming to us a full term before your rotation gives the sourcing and the paperwork room to land on schedule. Reach out through our contact form or WhatsApp/SMS with your track and region to begin.
Get matched with a
Purdue Global preceptor
Tell us your track, your city, and your term. We'll come back with a placement plan and a realistic date your affiliation agreement can clear by.